When nonprofits use multiple strategies during their online fundraising campaigns, such as thanking donors for their support, telling the public about their missions and conveying how they are helping people, they receive more donations than if they stick to only one kind of post.
We figured this out after analyzing data from 752 nonprofits that participated in Omaha Gives, an online 24-hour fundraising event in 2015 and 2020. While reviewing the Facebook posts shared during those events, which have since been discontinued, we saw that these appeals fell into six categories:
Beneficiaries: Explaining how the group helps people.
Goals: Encouraging donors to help reach a fundraising goal.
Gratitude: Thanking donors for their gifts.
Mission: Focusing on how the organization helps people.
Social media engagement: Asking donors to share the post or change their profile picture to boost the campaign.
Solicitation: Asking for donations.
We also considered the size of the nonprofits’ budgets, what they do, how long they’ve been operating, their prior experience in online fundraising, the total number of likes their Facebook profiles have garnered, the number of posts they made during the fundraising events, and how many times these posts were shared. The impact of having a mix of fundraising messages was consistent regardless of these other factors.
In addition to determining that using different types of messaging works best, we found that when nonprofits frequently share messages of gratitude or that highlight progress toward their goals, they tend to raise more money than if they just ask for donations.
Taking the strategy our study supports – making different kinds of posts – could help nonprofits beyond simply getting more donations. We suspect that it may also reduce donor fatigue. That is, it could make it less likely that donors will become so overwhelmed by the repetition of the same requests that they stop supporting a group they used to fund.
Online giving has grown in importance in recent years. It amounted to an estimated 12% of all nonprofit fundraising in 2023, the most recent year for which data is available. Social media campaigns are an important part of online fundraising strategies, even though nonprofits still raise much more money through email.
What still isn’t known
It’s unclear how much of what we found is specific to Facebook. Had we examined fundraising data from other social media platforms, the results might have been different. We also didn’t assess the nonprofits’ other fundraising activities, such as how engaged their board members were in these campaigns, or the extent of their other strategies, such as direct mail.
We aim to conduct a future study that will look at both offline and online fundraising efforts to isolate the impact of social media posts on fundraising.
The Research Brief is a short take about interesting academic work.
theconversation.com – Daniel Apai, Associate Dean for Research and Professor of Astronomy and Planetary Sciences, University of Arizona – 2025-04-18 17:44:00
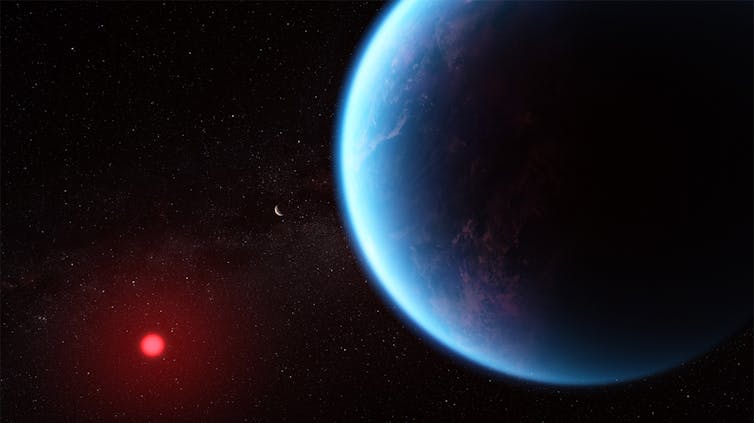
A team of astronomers announced on April 16, 2025, that in the process of studying a planet around another star, they had found evidence for an unexpected atmospheric gas. On Earth, that gas – called dimethyl sulfide – is mostly produced by living organisms.
In April 2024, the James Webb Space Telescope stared at the host star of the planet K2-18b for nearly six hours. During that time, the orbiting planet passed in front of the star. Starlight filtered through its atmosphere, carrying the fingerprints of atmospheric molecules to the telescope.
JWST’s cameras can detect molecules in the atmosphere of a planet by looking at light that passed through that atmosphere. European Space Agency
By comparing those fingerprints to 20 different molecules that they would potentially expect to observe in the atmosphere, the astronomers concluded that the most probable match was a gas that, on Earth, is a good indicator of life.
I am an astronomer and astrobiologist who studies planets around other stars and their atmospheres. In my work, I try to understand which nearby planets may be suitable for life.
K2-18b, a mysterious world
To understand what this discovery means, let’s start with the bizarre world it was found in. The planet’s name is K2-18b, meaning it is the first planet in the 18th planetary system found by the extended NASA Kepler mission, K2. Astronomers assign the “b” label to the first planet in the system, not “a,” to avoid possible confusion with the star.
K2-18b is a little over 120 light-years from Earth – on a galactic scale, this world is practically in our backyard.
Although astronomers know very little about K2-18b, we do know that it is very unlike Earth. To start, it is about eight times more massive than Earth, and it has a volume that’s about 18 times larger. This means that it’s only about half as dense as Earth. In other words, it must have a lot of water, which isn’t very dense, or a very big atmosphere, which is even less dense.
Astronomers think that this world could either be a smaller version of our solar system’s ice giant Neptune, called a mini-Neptune, or perhaps a rocky planet with no water but a massive hydrogen atmosphere, called a gas dwarf.
That term means hydrogen-over-ocean, since astronomers predict that hycean worlds are planets with global oceans many times deeper than Earth’s oceans, and without any continents. These oceans are covered by massive hydrogen atmospheres that are thousands of miles high.
Astronomers do not know yet for certain that hycean worlds exist, but models for what those would look like match the limited data JWST and other telescopes have collected on K2-18b.
This is where the story becomes exciting. Mini-Neptunes and gas dwarfs are unlikely to be hospitable for life, because they probably don’t have liquid water, and their interior surfaces have enormous pressures. But a hycean planet would have a large and likely temperate ocean. So could the oceans of hycean worlds be habitable – or even inhabited?
They found evidence for the presence of two simple carbon-bearing molecules – carbon monoxide and methane – and showed that the planet’s upper atmosphere lacked water vapor. This atmospheric composition supported, but did not prove, the idea that K2-18b could be a hycean world. In a hycean world, water would be trapped in the deeper and warmer atmosphere, closer to the oceans than the upper atmosphere probed by JWST observations.
Intriguingly, the data also showed an additional, very weak signal. The team found that this weak signal matched a gas called dimethyl sulfide, or DMS. On Earth, DMS is produced in large quantities by marine algae. It has very few, if any, nonbiological sources.
This signal made the initial detection exciting: on a planet that may have a massive ocean, there is likely a gas that is, on Earth, emitted by biological organisms.
Scientists had a mixed response to this initial announcement. While the findings were exciting, some astronomers pointed out that the DMS signal seen was weak and that the hycean nature of K2-18b is very uncertain.
To address these concerns, Mashusudhan’s team turned JWST back to K2-18b a year later. This time, they used another camera on JWST that looks for another range of wavelengths of light. The new results – announced on April 16, 2025 – supported their initial findings.
These new data show a stronger – but still relatively weak – signal that the team attributes to DMS or a very similar molecule. The fact that the DMS signal showed up on another camera during another set of observations made the interpretation of DMS in the atmosphere stronger.
Madhusudhan’s team also presented a very detailed analysis of the uncertainties in the data and interpretation. In real-life measurements, there are always some uncertainties. They found that these uncertainties are unlikely to account for the signal in the data, further supporting the DMS interpretation. As an astronomer, I find that analysis exciting.
Is life out there?
Does this mean that scientists have found life on another world? Perhaps – but we still cannot be sure.
First, does K2-18b really have an ocean deep beneath its thick atmosphere? Astronomers should test this.
Second, is the signal seen in two cameras two years apart really from dimethyl sulfide? Scientists will need more sensitive measurements and more observations of the planet’s atmosphere to be sure.
Third, if it is indeed DMS, does this mean that there is life? This may be the most difficult question to answer. Life itself is not detectable with existing technology. Astronomers will need to evaluate and exclude all other potential options to build their confidence in this possibility.
The new measurements may lead researchers toward a historic discovery. However, important uncertainties remain. Astrobiologists will need a much deeper understanding of K2-18b and similar worlds before they can be confident in the presence of DMS and its interpretation as a signature of life.
Scientists around the world are already scrutinizing the published study and will work on new tests of the findings, since independent verification is at the heart of science.
Moving forward, K2-18b is going to be an important target for JWST, the world’s most sensitive telescope. JWST may soon observe other potential hycean worlds to see if the signal appears in the atmospheres of those planets, too.
With more data, these tentative conclusions may not stand the test of time. But for now, just the prospect that astronomers may have detected gasses emitted by an alien ecosystem that bubbled up in a dark, blue-hued alien ocean is an incredibly fascinating possibility.
Regardless of the true nature of K2-18b, the new results show how using the JWST to survey other worlds for clues of alien life will guarantee that the next years will be thrilling for astrobiologists.
theconversation.com – Christina Erickson, Associate Dean in the College of Nursing and Professional Disciplines, University of North Dakota – 2025-04-18 07:39:00
Nearly a half-century after the Supreme Court ruled that school spankings are permissible and not “cruel and unusual punishment”, many U.S. states allow physical punishment for students who have misbehaved.
Christina Erickson, an associate dean and professor of social work at the University of North Dakota, wrote a book on the subject: “Spanked: How Hitting Our Children is Harming Ourselves.” She discussed the scope of the practice and its effects with The Conversation.
What spanking legislation exists worldwide?
Around the world, 68 countries have banned the hitting of children in any form, including spanking. This movement began in 1979 with Sweden’s ban on all forms of physical punishment, including spanking in any setting, and including in the family home.
Each state in the U.S. has its own child abuse laws, and all states, tribes and territories aim to protect children from abuse. But all state laws also allow parents to hit their children if it does not leave an injury or a mark.
A typical example is Oklahoma’s definition of child abuse and neglect. It includes an exception that permits parents to use ordinary force as a means of discipline, including spanking, using an implement like a switch or a paddle. However, leaving evidence of hitting, such as welts, bruises, swelling or lacerations, is illegal and considered child abuse in all states.
Parental spanking of children is considered unique from other physical violence because of the relational context and the purpose. Laws entitle parents to hit their children for the purpose of teaching a lesson or punishing them to improve behavior. Children are the only individuals in society who can be hit by another person and the law does not regard it as assault.
Spanking’s impact on a child is unfortunately similar to abusive hitting. Spanking has been labeled as an “Adverse Childhood Experience,” or ACE. These are events that cause poor health outcomes over the span of one’s life.
Some school districts require permission from parents to allow disciplinary paddling in school, while others do not require any communication. State law does not assure agreement between parents and school districts on what offenses warrant a paddling. Parents may feel they have no alternative but to keep their child in school, or fear reprisal from school administrators. Some students are old enough to denounce the punishment themselves.
In this school district, physical punishment is used only when parents give written permission.
Is spanking considered the same as hitting?
The term spank conceals the concept of hitting and is so commonplace it goes unquestioned, despite the fact that it is a grown adult hitting a person much smaller than them. The concept is further concealed because hitting a child’s bottom hides any injuries that may occur.
Types of hitting that are categorized as spanking have narrowed over the years but still persist. Some parents still use implements such as tree switches, wooden spoons, shoes or paddles to “spank” children, raising the chances for abuse.
Most spanking ends by the age of 12, partly because children this age are able to fight back. When a child turns 18, parental hitting becomes the same as hitting any other adult, a form of domestic violence or assault throughout the U.S.
There is a lack of a consistent understanding of what constitutes a spanking. The definition of spanking is unique to each family. The number of hits, clothed or not, or using an implement, all reflect geographical or familial differences in understanding what a spanking is.
How do US adults view spanking?
People in the United States generally accept spanking as part of raising children: 56% of U.S. adults strongly agree or agree that “… it is sometimes necessary to discipline a child with a good, hard spanking.” This view has been slowly changing since 1986, when 83% of adults agreed with that statement.
The laws worldwide that protect children from being hit usually begin by disallowing nonparental adults to hit children. This is happening in the U.S. too, where 31 states have banned paddling in schools.
With the slow but steady drop of parents who believe that sometimes children need a good hard spanking, as well as the ban of paddling in schools in 31 states, one could argue that the U.S. is moving toward a reduction in spanking.
What does research say about spanking?
Spanking’s negative influence on children’s behavior has been documented for decades. Spanking seems to work in the moment when it comes to changing or stopping the immediate behavior, but the negative effects are hidden in the short term and occur later in the child’s life. Yet because the spanking seemed to work at the time, the parent doesn’t connect the continued bad behavior of the child to the spanking.
No studies have shown positive long-term benefits from spanking. Because of the long-standing and expansive research findings showing a range of harm from spanking and the increased association with child abuse, the American Psychological Association recommends that parents should never spank their children.
What are some resources for parents?
Consider these questions when choosing a discipline method for your child:
Is the expectation of your child developmentally accurate? One of the most common reasons parents spank is because they are expecting a behavior the child is not developmentally able to execute.
Can the discipline you choose grow with your child? Nearly all spanking ends by age 12, when kids are big enough to fight back. Choose discipline methods you can use over the long term, such as additional chores, apologies, difficult conversations and others that can grow with your child.
Might there be another explanation for your child’s behavior? Difficulty of understanding, fear or miscommunication? Think of your child as a learner and use a growth mindset to help your child learn from their life experiences.
Parents are the leaders of their families. Good leaders show strength in nonthreatening ways, listen to others and explain their decisions. Don’t spoil your kids. But being firm does not have to include hitting.
Practicing calm when with your children will help you be calmer at work and in your other relationships. Listening to and speaking with a child about challenges, even from a very early age, is the best way to make it part of your relationship for the rest of your life.
Choose a method that allows you to grow. Parents matter too.
Every day, people are constantly learning and forming new memories. When you pick up a new hobby, try a recipe a friend recommended or read the latest world news, your brain stores many of these memories for years or decades.
But how does your brain achieve this incredible feat?
The human brain is made up of billions of nerve cells. These neurons conduct electrical pulses that carry information, much like how computers use binary code to carry data.
These electrical pulses are communicated with other neurons through connections between them called synapses. Individual neurons have branching extensions known as dendrites that can receive thousands of electrical inputs from other cells. Dendrites transmit these inputs to the main body of the neuron, where it then integrates all these signals to generate its own electrical pulses.
It is the collective activity of these electrical pulses across specific groups of neurons that form the representations of different information and experiences within the brain.
For decades, neuroscientists have thought that the brain learns by changing how neurons are connected to one another. As new information and experiences alter how neurons communicate with each other and change their collective activity patterns, some synaptic connections are made stronger while others are made weaker. This process of synaptic plasticity is what produces representations of new information and experiences within your brain.
In order for your brain to produce the correct representations during learning, however, the right synaptic connections must undergo the right changes at the right time. The “rules” that your brain uses to select which synapses to change during learning – what neuroscientists call the credit assignment problem – have remained largely unclear.
Defining the rules
We decided to monitor the activity of individual synaptic connections within the brain during learning to see whether we could identify activity patterns that determine which connections would get stronger or weaker.
To do this, we genetically encoded biosensors in the neurons of mice that would light up in response to synaptic and neural activity. We monitored this activity in real time as the mice learned a task that involved pressing a lever to a certain position after a sound cue in order to receive water.
We were surprised to find that the synapses on a neuron don’t all follow the same rule. For example, scientists have often thought that neurons follow what are called Hebbian rules, where neurons that consistently fire together, wire together. Instead, we saw that synapses on different locations of dendrites of the same neuron followed different rules to determine whether connections got stronger or weaker. Some synapses adhered to the traditional Hebbian rule where neurons that consistently fire together strengthen their connections. Other synapses did something different and completely independent of the neuron’s activity.
Our findings suggest that neurons, by simultaneously using two different sets of rules for learning across different groups of synapses, rather than a single uniform rule, can more precisely tune the different types of inputs they receive to appropriately represent new information in the brain.
In other words, by following different rules in the process of learning, neurons can multitask and perform multiple functions in parallel.
Future applications
This discovery provides a clearer understanding of how the connections between neurons change during learning. Given that most brain disorders, including degenerative and psychiatric conditions, involve some form of malfunctioning synapses, this has potentially important implications for human health and society.
For example, depression may develop from an excessive weakening of the synaptic connections within certain areas of the brain that make it harder to experience pleasure. By understanding how synaptic plasticity normally operates, scientists may be able to better understand what goes wrong in depression and then develop therapies to more effectively treat it.
These findings may also have implications for artificial intelligence. The artificial neural networks underlying AI have largely been inspired by how the brain works. However, the learning rules researchers use to update the connections within the networks and train the models are usually uniform and also not biologically plausible. Our research may provide insights into how to develop more biologically realistic AI models that are more efficient, have better performance, or both.
There is still a long way to go before we can use this information to develop new therapies for human brain disorders. While we found that synaptic connections on different groups of dendrites use different learning rules, we don’t know exactly why or how. In addition, while the ability of neurons to simultaneously use multiple learning methods increases their capacity to encode information, what other properties this may give them isn’t yet clear.
Future research will hopefully answer these questions and further our understanding of how the brain learns.