Mississippi Today
‘Desperate times’: Independent pharmacies fear closure, due in part to pharmacy benefit managers

Turnage Drug Store survived both world wars, the Great Depression, the rise of chain pharmacies and the decline in popularity of the soda fountain.
But the 119-year-old Water Valley pharmacy may now be facing its greatest threat yet: untenable reimbursement rates and non-negotiable contracts from pharmacy benefit managers, said co-owner Robert Turnage.
Turnage is one of many independent pharmacy owners in Mississippi who fear that if more stringent regulations are not imposed on pharmacy benefit managers, their businesses – some of the most accessible health care providers, particularly in rural parts of the state – may be forced to close.
“Everyone here is on the verge of closing their doors if something drastic is not done,” Bob Lomenick, the owner and pharmacist at Tyson Drugs, Inc. in Holly Springs, told lawmakers at the House Select Committee on Prescription Drugs meeting Aug. 21 at the Capitol. The meeting room was filled with independent pharmacists who came from around the state to plead their case with legislators.
Pharmacy benefit managers are private companies that serve as the middlemen between pharmacies, drug manufacturers and insurers. They negotiate pricing and conditions for access to drugs, process prescription claims and manage retail pharmacy networks.
A Federal Trade Commission report published in July sounded alarm bells about the companies’ “extraordinarily opaque” business practices and the considerable influence they exert upon independent pharmacies, or retail pharmacies not owned by a publicly traded company or affiliated with a large chain.
Pharmacy benefit managers’ anti-competitive business practices have increased prescription drug costs and diminished access to medicine and patient choice about which pharmacy to patronize, the report said.
U.S. Congress is also investigating the impact of pharmacy benefit managers’ business practices.
There are about 380 independent pharmacies in Mississippi, said Robert Dozier, the executive director of the Mississippi Independent Pharmacy Association, an organization that advocates for the interests of 180 pharmacy members.
A significant portion of Mississippi’s population, especially in rural areas where chain pharmacies are less likely to exist, is reliant on independent pharmacies, said Meagan Rosenthal, an associate professor in the University of Mississippi’s Department of Pharmacy Administration.
A pharmacy closure in a rural area is likely to create a pharmacy desert, or an area with limited or no access to a pharmacy. Research has shown that pharmacy closures have negative impacts on patients’ health, especially in medically underserved areas.
Over 300 pharmacies closed nationwide in 2023, said Joel Kurzman, the director of state government affairs for the National Community Pharmacists Association, a national organization that advocates for independent pharmacies.
“It’s a startling figure,” he said.

Shrinking reimbursements
Sharon Bonck, a pharmacist at Sartin’s Discount Drugs in Gulfport, said the rates pharmacies are paid for dispensing prescription drugs to patients with health insurance have dwindled over the past 10 years. In the past two or three years, however, the rates have become “disastrous” for business.
Some prescriptions yield negative, or “underwater,” reimbursements, or payments from health insurance plans that are less than the pharmacy’s cost to acquire the drug. Others don’t earn a profit high enough to meet the pharmacy’s average operating expenses.
Pharmacy benefit managers set reimbursement rates for pharmacies by contract. But independent pharmacies often do not have the leverage to negotiate the terms of the contracts.
“I’ve never, never, not one time, been able to negotiate a contract,” said Lomenick. “It’s take it or leave it. If I don’t take it, I won’t have patients coming into my store.”
Independent pharmacies are faced with a difficult decision: sign a contract that may not adequately compensate them for their service, or turn it down and lose customers.
As reimbursement payments for some health insurance plans have waned, pharmacists have begun to more often choose the latter.
Russell Love, the owner of Love’s Pharmacy, a chain of three pharmacies on the coast, said he stopped filling prescriptions for patients with TRICARE, a health insurance program for military service members and their families, and Magnolia Health’s Ambetter health insurance this year, also due to low reimbursement rates. Beginning in 2025, he will not accept Medicare Part D plans.
“A lot of veterans can’t get their meds at their local pharmacy,” said Todd Dear, associate director of the Mississippi Board of Pharmacy, at the legislative committee hearing Aug. 21.
TRICARE prescription claims are managed by Express Scripts, one the three largest pharmacy benefit managers in the country. Together, CVS Caremark, Express Scripts and OptumRx managed 79 percent of prescription drug claims for about 270 million Americans in 2023, according to the Federal Trade Commission’s report.
These three pharmacy benefit managers also own mail order and specialty pharmacies, health insurance plans, health care providers and companies that market and sell drugs, giving them “significant power over prescription drug access and prices,” wrote the federal agency’s findings.
The report also indicated that in some cases, pharmacy benefit managers reimburse their affiliate pharmacies at higher rates for specialty, high-cost drugs than for unaffiliated pharmacies.
Express Scripts executives told lawmakers that pharmacy benefit managers work to negotiate rebates with drug manufacturers that result in cost savings for employers who sponsor health plans.
“Pharmacy access is vital,” said Tony Grillo, Express Scripts’ vice president for supply chain finance. “We do need these independent pharmacists. There are a lot of communities in the state that are small and rural. There’s a lot of communities in this country that are small and rural. We need these pharmacies in our network. It’s not in our interest to put these folks out of business.”
Low reimbursement rates also impact what drugs Mississippians can access at independent pharmacies, like brand name drugs for diabetes and weight loss, including insulin, antidepressants and inhalers.
GLP-1 drugs, which are used to treat type 2 diabetes and weight loss, have some of the most untenable reimbursement rates, said pharmacist Michelle Little, the owner of Freedom Pharmacy in Hattiesburg. The loss for pharmacies, paired with supply shortages, makes them difficult for patients to access.
Mississippi has some of the highest diabetes and obesity rates in the country. Fifteen percent of Mississippians have been diagnosed with diabetes, and 40% are obese.
Little said she has been forced to turn patients away due to low reimbursement rates.
“It breaks our heart,” she said. “…We’re not able to service our patients and customers like we have been in the past.”

Limited health care access
Pharmacies may choose not to fill a prescription due to low reimbursement rates, but in other cases, pharmacy benefit managers restrict which pharmacies insured patients can visit by creating pharmacy networks.
Robert Turnage said some of his long-time patients’ insurance plans no longer allow them to fill their prescriptions at Turnage Drug Store. For Water Valley residents, that means a 60-minute round trip drive to Oxford, the closest town with major chain pharmacies.
“That absolutely has consequences for patients,” said Rosenthal, who said patients may choose to go without their medication to avoid driving long distances.
Pharmacies that participate in pharmacy benefit manager-designed networks usually agree to accept lower payments in exchange for a higher volume of patients, who are required to use an in-network pharmacy.
Pharmacists fear being kicked out of pharmacy benefit managers’ networks as retaliation for lodging complaints with the Mississippi Board of Pharmacy, the board’s executive director Susan McCoy told lawmakers Aug. 21.
But more and more, she said, pharmacists are coming forward due to the precarious position of their business.
“It’s getting desperate times,” McCoy said. “Our pharmacies are starting to come to us and say, ‘you know, it doesn’t matter if I get retaliated against, because I’m not going to be here anyway. Go ahead and do what you need to do to take action against the PBMs.’”
Reform attempts in Mississippi
Three states have passed laws setting reimbursement floors for prescription drugs and requiring transparency of drug pricing, said Kurzman. Several other states have regulations for their state health plans.
The Mississippi Legislature passed a law in 2020 that gave the Mississippi Board of Pharmacy additional authority to ensure that pharmacy benefit managers are following the law, including levying fines.
The board completed an audit of Optum Rx this year – the first pharmacy benefit manager the board has audited – but has not yet released its findings.
It took several years for the board to hire staff to carry out the law and receive approval for budget increases due to the high cost of audits, said McCoy.
But independent pharmacists say the law isn’t enough – setting minimum reimbursement rates and increasing price transparency are desperately needed reforms to ensure that pharmacies stay afloat.
For the past several years, state lawmakers have proposed legislation to further regulate pharmacy benefit managers.
In 2023, a bill that would have set minimum reimbursements for prescriptions at the national average drug acquisition cost, or NADAC, died in the House Insurance Committee, chaired by Rep. Jerry Turner, R-Baldwyn.
NADAC is a price index that approximates the amount pharmacies pay for prescription drugs.
But pharmacists argue NADAC as a baseline is not enough, because it does not factor in pharmacists’ dispensing and operational costs. Arkansas, which uses a NADAC pricing model, will require pharmacy benefit managers to include dispensing fees in their reimbursements to pharmacies, as a result of an emergency rule passed in September.
A 2024 bill that would have increased pricing transparency and prohibited pharmacy benefit managers from retaliating against pharmacies or charging insurance plans or patients more than the amount they paid pharmacies for a prescription died during the legislative session.
The House Select Committee on Prescription Drugs will make recommendations to the state Legislature after several more hearings.
“I’m optimistic that the State of Mississippi is going to do something,” said pharmacist Chris Bonner, the owner of Chris’ Pharmacy in Columbus. “It’s going to be too late for some people if they don’t do something soon.”
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.![]()














Mississippi Today
If Tate Reeves calls a tax cut special session, Senate has the option to do nothing

An illness is spreading through the Mississippi Capitol: special session fever.
Speculation is rampant that Gov. Tate Reeves will call a special session if the Senate does not acquiesce to his and the House leadership’s wishes to eliminate the state personal income tax.
Reeves and House leaders are fond of claiming that the about 30% of general fund revenue lost by eliminating the income tax can be offset by growth in other state tax revenue.
House leaders can produce fancy charts showing that the average annual 3% growth rate in state revenue collections can more than offset the revenue lost from a phase out of the income tax.
What is lost in the fancy charts is that the historical 3% growth rate in state revenue includes growth in the personal income tax, which is the second largest source of state revenue. Any growth rate will entail much less revenue if it does not include a 3% growth in the income tax, which would be eliminated if the governor and House leaders have their way. This is important because historically speaking, as state revenue grows so does the cost of providing services, from pay to state employees, to health care costs, to transportation costs, to utility costs and so on.
This does not even include the fact that historically speaking, many state entities providing services have been underfunded by the Legislature, ranging from education to health care, to law enforcement, to transportation. Again, the list goes on and on.
And don’t forget a looming $25 billion shortfall in the state’s Public Employee Retirement System that could create chaos at some point.
But should the Senate not agree to the elimination of the income tax and Reeves calls a special session, there will be tremendous pressure on the Senate leadership, particularly Lt. Gov. Delbert Hosemann, the chamber’s presiding officer.
Generally speaking, a special session will provide more advantages for the eliminate-the-income-tax crowd.
First off, it will be two against one. When the governor and one chamber of the Legislature are on the same page, it is often more difficult for the other chamber to prevail.
The Mississippi Constitution gives the governor sole authority to call a special session and set an agenda. But the Legislature does have discretion in how that agenda is carried out.
And the Legislature always has the option to do nothing during the special session. Simply adjourn and go home is an option.
But the state constitution also says if one chamber is in session, the other house cannot remain out of session for more than three days.
In other words, theoretically, the House and governor working together could keep the Senate in session all year.
In theory, senators could say they are not going to yield to the governor’s wishes and adjourn the special session. But if the House remained in session, the Senate would have to come back in three days. The Senate could then adjourn again, but be forced to come back if the House stubbornly remained in session.
The process could continue all year.
But in the real world, there does not appear to be a mechanism — constitutionally speaking — to force the Senate to come back. The Mississippi Constitution does say members can be “compelled” to attend a session in order to have a quorum, but many experts say that language would not be relevant to make an entire chamber return to session after members had voted to adjourn.
In the past, one chamber has failed to return to the Capitol and suffered no consequences after the other remained in session for more than three days.
As a side note, the Mississippi Constitution does give the governor the authority to end a special session should the two chambers not agree on adjournment. In the early 2000s, then-Gov. Ronnie Musgrove ended a special session when the House and Senate could not agree on a plan to redraw the state’s U.S. House districts to adhere to population shifts found by the U.S. Census.
But would Reeves want to end the special session without approval of his cherished income tax elimination plan?
Probably not.
In 2002 there famously was an 82-day special session to consider proposals to provide businesses more protection from lawsuits. No effort was made to adjourn that session. It just dragged on until the House finally agreed to a significant portion of the Senate plan to provide more lawsuit protection.
In 1969, a special session lasted most of the summer when the Legislature finally agreed to a proposal of then-Gov. John Bell Williams to opt into the federal Medicaid program.
In both those instances, those wanting something passed — Medicaid in the 1960s and lawsuit protections in the 2000s — finally prevailed.
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.![]()

Feb. 22, 1898

Frazier Baker, the first Black postmaster of the small town of Lake City, South Carolina, and his baby daughter, Julia, were killed, and his wife and three other daughters were injured when a lynch mob attacked.
When President William McKinley appointed Baker the previous year, local whites began to attack Baker’s abilities. Postal inspectors determined the accusations were unfounded, but that didn’t halt those determined to destroy him.
Hundreds of whites set fire to the post office, where the Bakers lived, and reportedly fired up to 100 bullets into their home. Outraged citizens in town wrote a resolution describing the attack and 25 years of “lawlessness” and “bloody butchery” in the area.
Crusading journalist Ida B. Wells wrote the White House about the attack, noting that the family was now in the Black hospital in Charleston “and when they recover sufficiently to be discharged, they) have no dollar with which to buy food, shelter or raiment.
McKinley ordered an investigation that led to charges against 13 men, but no one was ever convicted. The family left South Carolina for Boston, and later that year, the first nationwide civil rights organization in the U.S., the National Afro-American Council, was formed.
In 2019, the Lake City post office was renamed to honor Frazier Baker.
“We, as a family, are glad that the recognition of this painful event finally happened,” his great-niece, Dr. Fostenia Baker said. “It’s long overdue.”
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.![]()

by Justin Glowacki with contributions from Rasheed Ambrose, Javion Henry, McKenna Klamm, Matt Martin and Aidan Tarrant
BILOXI – On Feb. 1, Memorial Health System officially took over Merit Health Biloxi, solidifying its position as the dominant healthcare provider in the region. According to Fitch Ratings, Memorial now controls more than 85% of the local health care market.
This isn’t Memorial’s first hospital acquisition. In 2019, it took over Stone County Hospital and expanded services. Memorial considers that transition a success and expects similar results in Biloxi.
However, health care experts caution that when one provider dominates a market, it can lead to higher prices and fewer options for patients.
Expanding specialty care and services

One of the biggest benefits of the acquisition, according to Kristian Spear, the new administrator of Memorial Hospital Biloxi, will be access to Memorial’s referral network.
By joining Memorial’s network, Biloxi patients will have access to more services, over 40 specialties and over 100 clinics.
“Everything that you can get at Gulfport, you will have access to here through the referral system,” Spear said.
One of the first improvements will be the reopening of the Radiation Oncology Clinic at Cedar Lake, which previously shut down due to “availability shortages,” though hospital administration did not expand on what that entailed.
“In the next few months, the community will see a difference,” Spear said. “We’re going to bring resources here that they haven’t had.”
Beyond specialty care, Memorial is also expanding hospital services and increasing capacity. Angela Benda, director of quality and performance improvement at Memorial Hospital Biloxi, said the hospital is focused on growth.
“We’re a 153-bed hospital, and we average a census of right now about 30 to 40 a day. It’s not that much, and so, the plan is just to grow and give more services,” Benda said. “So, we’re going to expand on the fifth floor, open up more beds, more admissions, more surgeries, more provider presence, especially around the specialties like cardiology and OB-GYN and just a few others like that.”
For patient Kenneth Pritchett, a Biloxi resident for over 30 years, those changes couldn’t come soon enough.

Pritchett, who was diagnosed with congestive heart failure, received treatment at Merit Health Biloxi. He currently sees a cardiologist in Cedar Lake, a 15-minute drive on the interstate. He says having a cardiologist in Biloxi would make a difference.
“Yes, it’d be very helpful if it was closer,” Pritchett said. “That’d be right across the track instead of going on the interstate.”
Beyond specialty services and expanded capacity, Memorial is upgrading medical equipment and renovating the hospital to improve both function and appearance. As far as a timeline for these changes, Memorial said, “We are taking time to assess the needs and will make adjustments that make sense for patient care and employee workflow as time and budget allow.”
Unanswered questions: insurance and staffing
As Memorial Health System takes over Merit Health Biloxi, two major questions remain:
- Will patients still be covered under the same insurance plans?
- Will current hospital staff keep their jobs?
Insurance Concerns
Memorial has not finalized agreements with all insurance providers and has not provided a timeline for when those agreements will be in place.
In a statement, the hospital said:
“Memorial recommends that patients contact their insurance provider to get their specific coverage questions answered. However, patients should always seek to get the care they need, and Memorial will work through the financial process with the payers and the patients afterward.”
We asked Memorial Health System how the insurance agreements were handled after it acquired Stone County Hospital. They said they had “no additional input.”
What about hospital staff?
According to Spear, Merit Health Biloxi had around 500 employees.
“A lot of the employees here have worked here for many, many years. They’re very loyal. I want to continue that, and I want them to come to me when they have any concerns, questions, and I want to work with this team together,” Spear said.
She explained that there will be a 90-day transitional period where all employees are integrated into Memorial Health System’s software.
“Employees are not going to notice much of a difference. They’re still going to come to work. They’re going to do their day-to-day job. Over the next few months, we will probably do some transitioning of their computer system. But that’s not going to be right away.”
The transition to new ownership also means Memorial will evaluate how the hospital is operated and determine if changes need to be made.
“As we get it and assess the different workflows and the different policies, there will be some changes to that over time. Just it’s going to take time to get in here and figure that out.”
During this 90-day period, Erin Rosetti, Communications Manager at Memorial Health System said, “Biloxi employees in good standing will transition to Memorial at the same pay rate and equivalent job title.”
Kent Nicaud, President and CEO of Memorial Health System, said in a statement that the hospital is committed to “supporting our staff and ensuring they are aligned with the long-term vision of our health system.”
What research says about hospital consolidations
While Memorial is promising improvements, larger trends in hospital mergers raise important questions.
Research published by the Rand Corporation, a nonprofit, nonpartisan research organization, found that research into hospital consolidations reported increased prices anywhere from 3.9% to 65%, even among nonprofit hospitals.
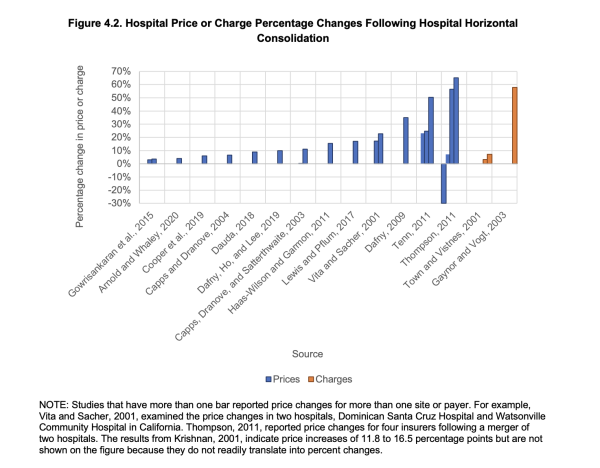
The impact on patient care is mixed. Some studies suggest merging hospitals can streamline services and improve efficiency. Others indicate mergers reduce competition, which can drive up costs without necessarily improving care.
When asked about potential changes to the cost of care, hospital leaders declined to comment until after negations with insurance companies are finalized, but did clarify Memorial’s “prices are set.”
“We have a proven record of being able to go into institutions and transform them,” said Angie Juzang, Vice President of Marketing and Community Relations at Memorial Health System.
When Memorial acquired Stone County Hospital, it expanded the emergency room to provide 24/7 emergency room coverage and renovated the interior.
When asked whether prices increased after the Stone County acquisition, Memorial responded:
“Our presence has expanded access to health care for everyone in Stone County and the surrounding communities. We are providing quality healthcare, regardless of a patient’s ability to pay.”
The response did not directly address whether prices went up — leaving the question unanswered.
The bigger picture: Hospital consolidations on the rise
According to health care consulting firm Kaufman Hall, hospital mergers and acquisitions are returning to pre-pandemic levels and are expected to increase through 2025.
Hospitals are seeking stronger financial partnerships to help expand services and remain stable in an uncertain health care market.
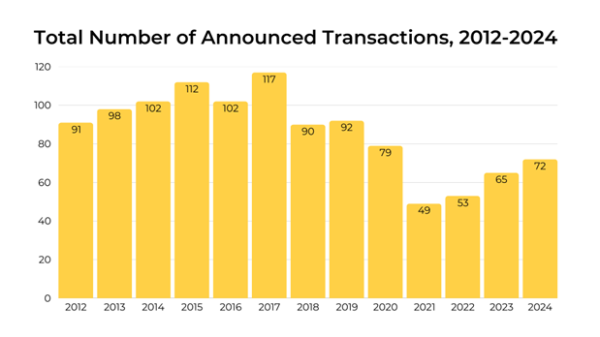
Source: Kaufman Hall M&A Review
Proponents of hospital consolidations argue mergers help hospitals operate more efficiently by:
- Sharing resources.
- Reducing overhead costs.
- Negotiating better supply pricing.
However, opponents warn few competitors in a market can:
- Reduce incentives to lower prices.
- Slow wage increases for hospital staff.
- Lessen the pressure to improve services.
Leemore Dafny, PhD, a professor at Harvard and former deputy director for health care and antitrust at the Federal Trade Commission’s Bureau of Economics, has studied hospital consolidations extensively.
In testimony before Congress, she warned: “When rivals merge, prices increase, and there’s scant evidence of improvements in the quality of care that patients receive. There is also a fair amount of evidence that quality of care decreases.”
Meanwhile, an American Hospital Association analysis found consolidations lead to a 3.3% reduction in annual operating expenses and a 3.7% reduction in revenue per patient.
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.![]()

Potential measles exposure reported in San Antonio, San Marcos

MCSO: Man arrested, charged after 3 shot at The Woodlands pub

A break in the freezing temps draws St. Louisans outdoors

Elon Musk email federal workers to explain what they did last week

Pirates Run Aground In Morton’s 38-32 State Quarterfinal Victory

‘You react’: Hope Mills first responders talk about courage summoned in water rescue

Man paroled after killing father, stepmother deceased in Rankin County crash

Senate passes SB 460 allowing vaccine exemptions; House delegates express mixed reactions

Bill to limit wind farms in 48 counties jumps to new committee

Quieter Weather Week Ahead; Early March Changes On The Horizon

Jeff Landry’s budget includes cuts to Louisiana’s domestic violence shelter funding

Bills from NC lawmakers expand gun rights, limit cellphone use

Modest drops in some North Carolina prices under Trump | North Carolina

Timing out the incoming winter weather

Remains of Aubrey Dameron found, family gathers in her honor

Expert discusses how deportations could cause labor shortages for several industries

ICE charges Texas bakery owners with harboring immigrants

SC Flu cases on the rise: Prisma Health Doctors speak out on how to spot symptoms, get treatment

Mississippi could face health research funding cuts under Trump administration policy

Trump says AP will continue to be curtailed at White House until it changes style to Gulf of America
Potential measles exposure reported in San Antonio, San Marcos
MCSO: Man arrested, charged after 3 shot at The Woodlands pub
A break in the freezing temps draws St. Louisans outdoors
Elon Musk email federal workers to explain what they did last week
‘You react’: Hope Mills first responders talk about courage summoned in water rescue
Senate passes SB 460 allowing vaccine exemptions; House delegates express mixed reactions
Bill to limit wind farms in 48 counties jumps to new committee
Quieter Weather Week Ahead; Early March Changes On The Horizon

FIRST ALERT: Weekly forecast and Mardi Gras temperatures with Aaron Colby (2/23/2025)

Behind the Business: Beautiful Minds Childcare
-

 News from the South - Louisiana News Feed3 days ago
News from the South - Louisiana News Feed3 days agoJeff Landry’s budget includes cuts to Louisiana’s domestic violence shelter funding
-
News from the South - North Carolina News Feed3 days ago
Bills from NC lawmakers expand gun rights, limit cellphone use
-
News from the South - North Carolina News Feed7 days ago
Modest drops in some North Carolina prices under Trump | North Carolina
-
News from the South - Arkansas News Feed7 days ago
Timing out the incoming winter weather
-
News from the South - Oklahoma News Feed5 days ago
Remains of Aubrey Dameron found, family gathers in her honor
-
News from the South - Texas News Feed3 days ago
ICE charges Texas bakery owners with harboring immigrants
-
News from the South - Florida News Feed7 days ago
Expert discusses how deportations could cause labor shortages for several industries
-
News from the South - South Carolina News Feed6 days ago
SC Flu cases on the rise: Prisma Health Doctors speak out on how to spot symptoms, get treatment