In space, there are clouds that contain gas and dust ejected from stars. Our solar system was formed 4.6 billion years ago from such a molecular cloud. Most of these dust grains were destroyed during solar system formation. However, a very small amount of the grains survived and remained intact in primitive meteorites. They are called presolar grains because they predate the solar system. I am a scientist who studies the early solar system and beyond, focusing mainly on presolar grains.
The picture is an image of such a grain taken by a scanning electron microscope. This grain is silicon carbide (SiC). The scale bar is 1 micron, or one millionth of a meter (39.37 inches). The grain was extracted from the Murchison meteorite that fell in Australia in 1969.
A fragment of the Murchison meteorite from which the grain was extracted, hosted at the National Museum of Natural History in Washington, D.C.
Scientists have investigated physical properties of the grain to determine its origin. Carbon has two stable isotopes, ¹²C and ¹³C, whose weights are slightly different from one another. The ratio between these isotopes is almost unchanged by processes taking place in the solar system such as evaporation and condensation. In contrast, nucleosynthetic processes in stars cause ¹²C/¹³C ratios to vary from 1 to over 200,000.
If this grain had originated within the solar system, its ¹²C/¹³C ratio would be 89. The ¹²C/¹³C ratio of the grain in this picture is about 55.1, which attests to its stellar origin. Together with other information about the grain, the ratio tells us that this grain formed in a type of star called an asymptotic giant branch star. The star was at the end of its life cycle when it profusely produced and expelled dust into space more than 4.6 billion years ago.
Scientists have found other types of presolar grains in meteorites, including diamond, graphite, oxides and silicates. Presolar grains like the one in the picture help researchers understand nucleosynthesis in stars, mixing of different zones in stars and stellar ejecta, and how abundances of elements and their isotopes change with time in the galaxy.
Contaminated milk from one plant in Illinois sickened thousands with Salmonella in 1985 − as outbreaks rise in the US, lessons from this one remain true
theconversation.com – Michael Petros, Clinical Assistant Professor of Environmental and Occupational Health Sciences, University of Illinois Chicago – 2025-05-07 07:34:00
A valve that mixed raw milk with pasteurized milk at Hillfarm Dairy may have been the source of contamination. This was the milk processing area of the plant. AP Photo/Mark Elias
In 1985, contaminated milk in Illinois led to a Salmonella outbreak that infected hundreds of thousands of people across the United States and caused at least 12 deaths. At the time, it was the largest single outbreak of foodborne illness in the U.S. and remains the worst outbreak of Salmonella food poisoning in American history.
Many questions circulated during the outbreak. How could this contamination occur in a modern dairy farm? Was it caused by a flaw in engineering or processing, or was this the result of deliberate sabotage? What roles, if any, did politics and failed leadership play?
From my 50 years of working in public health, I’ve found that reflecting on the past can help researchers and officials prepare for future challenges. Revisiting this investigation and its outcome provides lessons on how food safety inspections go hand in hand with consumer protection and public health, especially as hospitalizations and deaths from foodborne illnesses rise.
Contamination, investigation and intrigue
The Illinois Department of Public Health and the U.S. Centers for Disease Control and Prevention led the investigation into the outbreak. The public health laboratories of the city of Chicago and state of Illinois were also closely involved in testing milk samples.
Investigators and epidemiologists from local, state and federal public health agencies found that specific lots of milk with expiration dates up to April 17, 1985, were contaminated with Salmonella. The outbreak may have been caused by a valve at a processing plant that allowed pasteurized milk to mix with raw milk, which can carry several harmful microorganisms, including Salmonella.
Overall, labs and hospitals in Illinois and five other Midwest states – Indiana, Iowa, Michigan, Minnesota and Wisconsin – reported over 16,100 cases of suspected Salmonella poisoning to health officials.
To make dairy products, skimmed milk is usually separated from cream, then blended back together in different levels to achieve the desired fat content. While most dairies pasteurize their products after blending, Hillfarm Dairy in Melrose Park, Illinois, pasteurized the milk first before blending it into various products such as skim milk and 2% milk.
Subsequent examination of the production process suggested that Salmonella may have grown in the threads of a screw-on cap used to seal an end of a mixing pipe. Investigators also found this strain of Salmonella 10 months earlier in a much smaller outbreak in the Chicago area.
The contaminated milk was produced at Hillfarm Dairy in Melrose Park, which was operated at the time by Jewel Companies Inc. During an April 3 inspection of the company’s plant, the Food and Drug Administration found 13 health and safety violations.
The legal fallout of the outbreak expanded when the Illinois attorney general filed suit against Jewel Companies Inc., alleging that employees at as many as 18 stores in the grocery chain violated water pollution laws when they dumped potentially contaminated milk into storm sewers. Later, a Cook County judge found Jewel Companies Inc. in violation of the court order to preserve milk products suspected of contamination and maintain a record of what happened to milk returned to the Hillfarm Dairy.
Political fallout also ensued. The Illinois governor at the time, James Thompson, fired the director of the Illinois Public Health Department when it was discovered that he was vacationing in Mexico at the onset of the outbreak and failed to return to Illinois. Notably, the health director at the time of the outbreak was not a health professional. Following this episode, the governor appointed public health professional and medical doctor Bernard Turnock as director of the Illinois Department of Public Health.
In 1987, after a nine-month trial, a jury determined that Jewel officials did not act recklessly when Salmonella-tainted milk caused one of the largest food poisoning outbreaks in U.S. history. No punitive damages were awarded to victims, and the Illinois Appellate Court later upheld the jury’s decision.
Raw milk is linked to many foodborne illnesses.
Lessons learned
History teaches more than facts, figures and incidents. It provides an opportunity to reflect on how to learn from past mistakes in order to adapt to future challenges. The largest Salmonella outbreak in the U.S. to date provides several lessons.
For one, disease surveillance is indispensable to preventing outbreaks, both then and now. People remain vulnerable to ubiquitous microorganisms such as Salmonella and E. coli, and early detection of an outbreak could stop it from spreading and getting worse.
Additionally, food production facilities can maintain a safe food supply with careful design and monitoring. Revisiting consumer protections can help regulators keep pace with new threats from new or unfamiliar pathogens.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
The article provides an analytical, factual recounting of the 1985 Salmonella outbreak, with an emphasis on public health, safety standards, and lessons learned from past mistakes. It critiques the failures in leadership and oversight during the incident but avoids overt ideological framing. While it highlights political accountability, particularly the firing of a public health official and the appointment of a medical professional, it does so in a balanced manner without assigning blame to a specific political ideology. The content stays focused on the public health aspect and the importance of professional leadership, reflecting a centrist perspective in its delivery.
The 2002 sci-fi thriller “Minority Report” depicted a dystopian future where a specialized police unit was tasked with arresting people for crimes they had not yet committed. Directed by Steven Spielberg and based on a short story by Philip K. Dick, the drama revolved around “PreCrime” − a system informed by a trio of psychics, or “precogs,” who anticipated future homicides, allowing police officers to intervene and prevent would-be assailants from claiming their targets’ lives.
The film probes at hefty ethical questions: How can someone be guilty of a crime they haven’t yet committed? And what happens when the system gets it wrong?
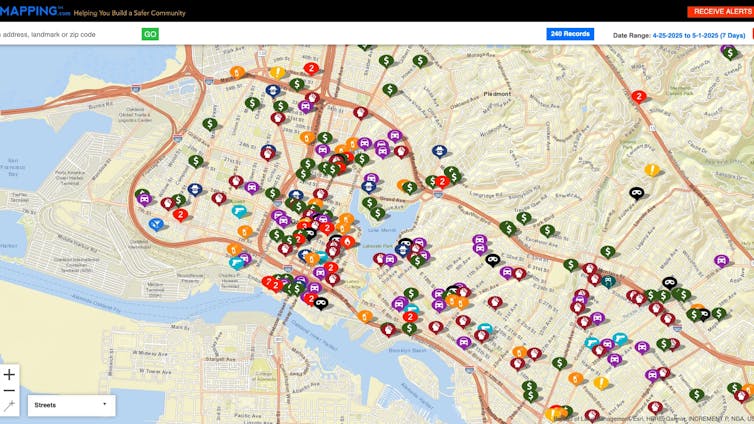
While there is no such thing as an all-seeing “precog,” key components of the future that “Minority Report” envisioned have become reality even faster than its creators imagined. For more than a decade, police departments across the globe have been using data-driven systems geared toward predicting when and where crimes might occur and who might commit them.
Far from an abstract or futuristic conceit, predictive policing is a reality. And market analysts are predicting a boom for the technology.
Predictive policing relies on artificial intelligence and data analytics to anticipate potential criminal activity before it happens. It can involve analyzing large datasets drawn from crime reports, arrest records and social or geographic information to identify patterns and forecast where crimes might occur or who may be involved.
Law enforcement agencies have used data analytics to track broad trends for many decades. Today’s powerful AI technologies, however, take in vast amounts of surveillance and crime report data to provide much finer-grained analysis.
Police departments use these techniques to help determine where they should concentrate their resources. Place-based prediction focuses on identifying high-risk locations, also known as hot spots, where crimes are statistically more likely to happen. Person-based prediction, by contrast, attempts to flag individuals who are considered at high risk of committing or becoming victims of crime.
These types of systems have been the subject of significant public concern. Under a so-called “intelligence-led policing” program in Pasco County, Florida, the sheriff’s department compiled a list of people considered likely to commit crimes and then repeatedly sent deputies to their homes. More than 1,000 Pasco residents, including minors, were subject to random visits from police officers and were cited for things such as missing mailbox numbers and overgrown grass.
Lawsuits forced the Pasco County, Fla., Sheriff’s Office to end its troubled predictive policing program.
Four residents sued the county in 2021, and last year they reached a settlement in which the sheriff’s office admitted that it had violated residents’ constitutional rights to privacy and equal treatment under the law. The program has since been discontinued.
This is not just a Florida problem. In 2020, Chicago decommissioned its “Strategic Subject List,” a system where police used analytics to predict which prior offenders were likely to commit new crimes or become victims of future shootings. In 2021, the Los Angeles Police Department discontinued its use of PredPol, a software program designed to forecast crime hot spots but was criticized for low accuracy rates and reinforcing racial and socioeconomic biases.
Necessary innovations or dangerous overreach?
The failure of these high-profile programs highlights a critical tension: Even though law enforcement agencies often advocate for AI-driven tools for public safety, civil rights groups and scholars have raised concerns over privacy violations, accountability issues and the lack of transparency. And despite these high-profile retreats from predictive policing, many smaller police departments are using the technology.
Most American police departments lack clear policies on algorithmic decision-making and provide little to no disclosure about how the predictive models they use are developed, trained or monitored for accuracy or bias. A Brookings Institution analysis found that in many cities, local governments had no public documentation on how predictive policing software functioned, what data was used, or how outcomes were evaluated.
Predictive policing can perpetuate racial bias.
This opacity is what’s known in the industry as a “black box.” It prevents independent oversight and raises serious questions about the structures surrounding AI-driven decision-making. If a citizen is flagged as high-risk by an algorithm, what recourse do they have? Who oversees the fairness of these systems? What independent oversight mechanisms are available?
These questions are driving contentious debates in communities about whether predictive policing as a method should be reformed, more tightly regulated or abandoned altogether. Some people view these tools as necessary innovations, while others see them as dangerous overreach.
A better way in San Jose
But there is evidence that data-driven tools grounded in democratic values of due process, transparency and accountability may offer a stronger alternative to today’s predictive policing systems. What if the public could understand how these algorithms function, what data they rely on, and what safeguards exist to prevent discriminatory outcomes and misuse of the technology?
The city of San Jose, California, has embarked on a process that is intended to increase transparency and accountability around its use of AI systems. San Jose maintains a set of AI principles requiring that any AI tools used by city government be effective, transparent to the public and equitable in their effects on people’s lives. City departments also are required to assess the risks of AI systems before integrating them into their operations.
If taken correctly, these measures can effectively open the black box, dramatically reducing the degree to which AI companies can hide their code or their data behind things such as protections for trade secrets. Enabling public scrutiny of training data can reveal problems such as racial or economic bias, which can be mitigated but are extremely difficult if not impossible to eradicate.
Research has shown that when citizens feel that government institutions act fairly and transparently, they are more likely to engage in civic life and support public policies. Law enforcement agencies are likely to have stronger outcomes if they treat technology as a tool – rather than a substitute – for justice.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Center-Left
The article provides an analysis of predictive policing, highlighting both the technological potential and ethical concerns surrounding its use. While it presents factual information, it leans towards caution and skepticism regarding the fairness, transparency, and potential racial biases of these systems. The framing of these issues, along with an emphasis on democratic accountability, transparency, and civil rights, aligns more closely with center-left perspectives that emphasize government oversight, civil liberties, and fairness. The critique of predictive policing technologies without overtly advocating for their abandonment reflects a balanced but cautious stance on technology’s role in law enforcement.
Evolution has fostered many reproductive strategies across the spectrum of life. From dandelions to giraffes, nature finds a way.
One of those ways creates quite a bit of suffering for humans: pollen, the infamous male gametophyte of the plant kingdom.
In the Southeastern U.S., where I live, you know it’s spring when your car has turned yellow and pollen blankets your patio furniture and anything else left outside. Suddenly there are long lines at every car wash in town.
Even people who aren’t allergic to pollen – clearly an advantage for a pollination ecologist like me – can experience sneezing and watery eyes during the release of tree pollen each spring. Enough particulate matter in the air will irritate just about anyone, even if your immune system does not launch an all-out attack.
So, why is there so much pollen? And why does it seem to be getting worse?
2 ways trees spread their pollen
Trees don’t have an easy time in the reproductive game. As a tree, you have two options to disperse your pollen.
Option 1: Employ an agent, such as a butterfly or bee, that can carry your pollen to another plant of the same species.
The downside of this option is that you must invest in a showy flower display and a sweet scent to advertise yourself, and sugary nectar to pay your agent for its services.
A bee enjoys pollen from a cherry blossom. Pollen is a primary source of protein for bees. Ivan Radic/Flickr, CC BY
Option 2, the budget option, is much less precise: Get a free ride on the wind.
Wind was the original pollinator, evolving long before animal-mediated pollination. Wind doesn’t require a showy flower nor a nectar reward. What it does require for pollination to succeed is ample amounts of lightweight, small-diameter pollen.
Why wind-blown pollen makes allergies worse
Wind is not an efficient pollinator, however. The probability of one pollen grain landing in the right location – the stigma or ovule of another plant of the same species – is infinitesimally small.
Therefore, wind-pollinated trees must compensate for this inefficiency by producing copious amounts of pollen, and it must be light enough to be carried.
For allergy sufferers, that can mean air filled with microscopic pollen grains that can get into your eyes, throat and lungs, sneak in through window screens and convince your immune system that you’ve inhaled a dangerous intruder.
Plants relying on animal-mediated pollination, by contrast, can produce heavier and stickier pollen to adhere to the body of an insect. So don’t blame the bees for your allergies – it’s really the wind.
Climate change has a role here, too
Plants initiate pollen release based on a few factors, including temperature and light cues. Many of our temperate tree species respond to cues that signal the beginning of spring, including warmer temperatures.
Studies have found that pollen seasons have intensified in the past three decades as the climate has warmed. One study that examined 60 location across North America found pollen seasons expanded by an average of 20 days from 1990 to 2018 and pollen concentrations increased by 21%.
Anyone who has lived in the Southeast for the past couple of decades has likely noticed this. The region has more tornado warnings, more severe thunderstorms, more power outages. This is especially true in the mid-South, from Mississippi to Alabama.
Severity of wind and storm events mapped from NOAA data, 2012-2019, shows high activity over Mississippi and Alabama. Red areas have the most severe events. Christine Cairns Fortuin
Since wind is the vector of airborne pollen, windier conditions can also make allergies worse. Pollen remains airborne for longer on windy days, and it travels farther.
To make matters worse, increasing storm activity may be doing more than just transporting pollen. Storms can also break apart pollen grains, creating smaller particles that can penetrate deeper into the lungs.
Many allergy sufferers may notice worsening allergies during storms.
The peak of spring wind and storm season tends to correspond to the timing of the release of tree pollen that blankets our world in yellow. The effects of climate change, including longer pollen seasons and more pollen released, and corresponding shifts in windy days and storm severity are helping to create the perfect pollen storm.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
The content is a scientific and educational article focusing on the biology of pollen, its effects on allergies, and the influence of climate change on pollen production. It presents factual information supported by research studies and references, without taking a partisan stance. While it acknowledges climate change as a factor, the discussion remains grounded in scientific observation rather than political opinion, leading to a neutral, centrist tone.