Prohibition is a must-do subject. Students expect it. But I cover several hundred years of history: from the 17th-century invention of rum – as a byproduct of sugar produced by enslaved people – to the rise of craft beer and craft spirits in the 21st century.
Along the way, I’m thrilled when students get excited about details that allow them to taste a more complicated historical cocktail. For example, they learn why white women’s production of hard cider was crucial to the survival of colonial Virginia. The short answer: Potable water was in short supply, alcoholic drinks were far healthier, and white men – and their indentured and enslaved workforce – were busy raising tobacco. It fell to women to turn fruit into salvation.
Why is this course relevant now?
Alcohol remains a big and almost inescapable part of American society. But of late, Americans have been drinking differently – and thinking about drinking differently.
Alcohol has been a highly controversial, central aspect of the American experience, shaping virtually all sectors of our society – political and constitutional, business and economic, social and cultural.
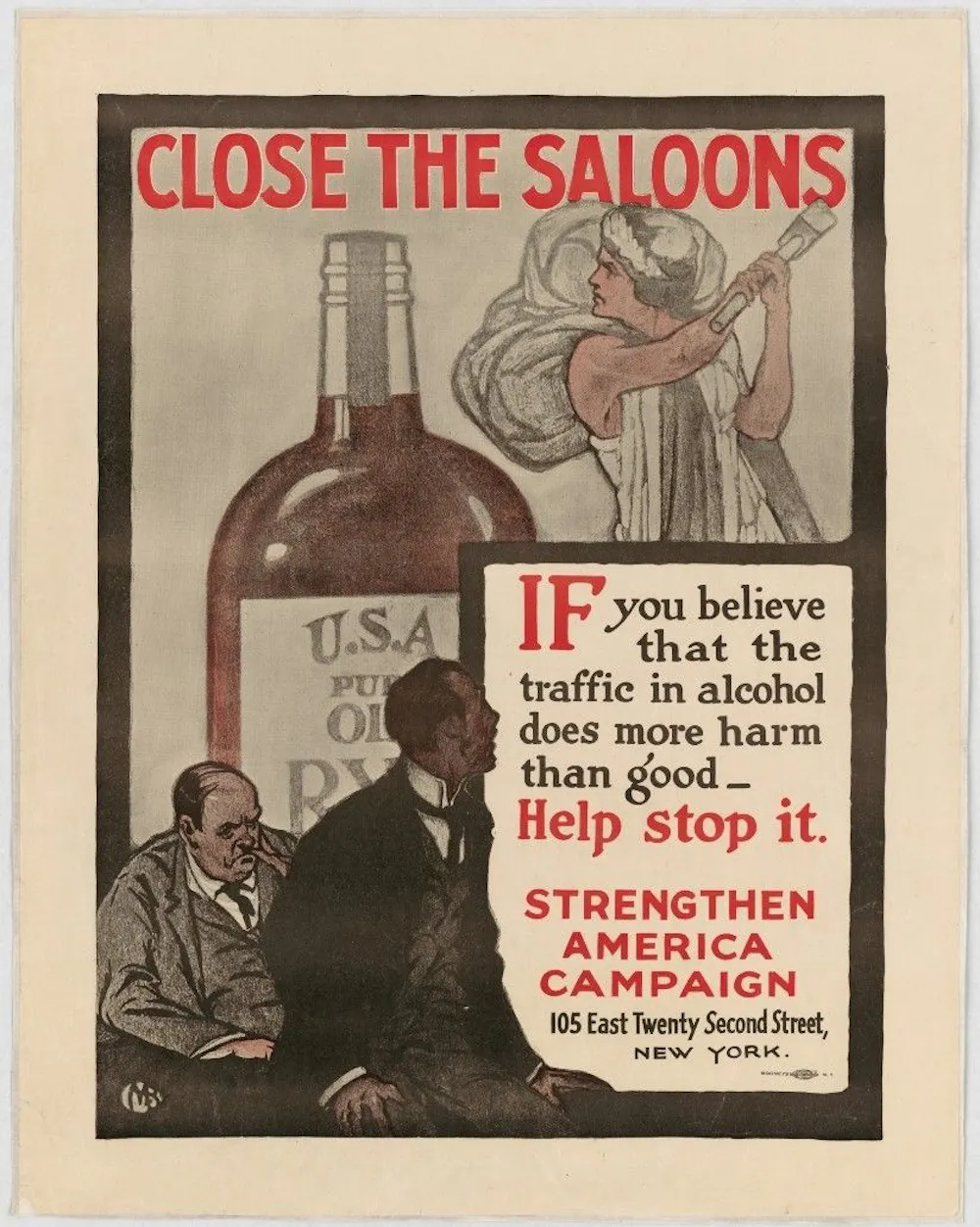
Jack London’s alcoholic memoir, “John Barleycorn”: a deep dive into the notorious workingmen’s saloons of the industrial era, as well as one person’s reckoning with alcoholism
“Days of Wine and Roses”: the 1962 film starring Jack Lemmon and Lee Remick that spotlighted the place of alcoholic marriages and Alcoholics Anonymous in post-World War II America
Like any history course, this one aims to develop student’s analytical, written, research and verbal skills. In lots of ways, the topic is just a tool to get students to grow their brains. But I also seek to grow students’ critical awareness of the place of alcohol in their own lives. The course has also informed students’ paths after graduation – including some who wound up working in the alcohol industry or recovery organizations.
Is your green my green? Probably not. What appears as pure green to me will likely look a bit yellowish or blueish to you. This is because visual systems vary from person to person. Moreover, an object’s color may appear differently against different backgrounds or under different lighting.
These facts might naturally lead you to think that colors are subjective. That, unlike features such as length and temperature, colors are not objective features. Either nothing has a true color, or colors are relative to observers and their viewing conditions.
There is a surprising amount of variation in how people perceive the world. If you offer a group of people a spectrum of color chips ranging from chartreuse to purple and asked them to pick the unique green chip – the chip with no yellow or blue in it – their choices would vary considerably. Indeed, there wouldn’t be a single chip that most observers would agree is unique green.
Generally, an object’s background can result in dramatic changes in how you perceive its colors. If you place a gray object against a lighter background, it will appear darker than if you place it against a darker background. This variation in perception is perhaps most striking when viewing an object under different lighting, where a red apple could look green or blue.
Of course, that you experience something differently does not prove that what is experienced is not objective. Water that feels cold to one person may not feel cold to another. And although we do not know who is feeling the water “correctly,” or whether that question even makes sense, we can know the temperature of the water and presume that this temperature is independent of your experience.
Similarly, that you can change the appearance of something’s color is not the same as changing its color. You can make an apple look green or blue, but that is not evidence that the apple is not red.
For comparison, the Moon appears larger when it’s on the horizon than when it appears near its zenith. But the size of the Moon has not changed, only its appearance. Hence, that the appearance of an object’s color or size varies is, by itself, no reason to think that its color and size are not objective features of the object. In other words, the properties of an object are independent of how they appear to you.
That said, given that there is so much variation in how objects appear, how do you determine what color something actually is? Is there a way to determine the color of something despite the many different experiences you might have of it?
Matching colors
Perhaps determining the color of something is to determine whether it is red or blue. But we suggest a different approach. Notice that squares that appear to be the same shade of pink against different backgrounds look different against the same background.
The smaller squares may appear to be the same color, but if you compare them with the strip of squares at the bottom, they’re actually different shades. Shobdohin/Wikimedia Commons, CC BY-SA
It’s easy to assume that to prove colors are objective would require knowing which observers, lighting conditions and backgrounds are the best, or “normal.” But determining the right observers and viewing conditions is not required for determining the very specific color of an object, regardless of its name. And it is not required to determine whether two objects have the same color.
To determine whether two objects have the same color, an observer would need to view the objects side by side against the same background and under various lighting conditions. If you painted part of a room and find that you don’t have enough paint, for instance, finding a match might be very tricky. A color match requires that no observer under any lighting condition will see a difference between the new paint and the old.
Is the dress yellow and white or black and blue?
That two people can determine whether two objects have the same color even if they don’t agree on exactly what that color is – just as a pool of water can have a particular temperature without feeling the same to me and you – seems like compelling evidence to us that colors are objective features of our world.
Colors, science and indispensability
Everyday interactions with colors – such as matching paint samples, determining whether your shirt and pants clash, and even your ability to interpret works of art – are hard to explain if colors are not objective features of objects. But if you turn to science and look at the many ways that researchers think about colors, it becomes harder still.
For example, in the field of color science, scientific laws are used to explain how objects and light affect perception and the colors of other objects. Such laws, for instance, predict what happens when you mix colored pigments, when you view contrasting colors simultaneously or successively, and when you look at colored objects in various lighting conditions.
The philosophers Hilary Putnam and Willard van Orman Quine made famous what is known as the indispensability argument. The basic idea is that if something is indispensable to science, then it must be real and objective – otherwise, science wouldn’t work as well as it does.
For example, you may wonder whether unobservable entities such as electrons and electromagnetic fields really exist. But, so the argument goes, the best scientific explanations assume the existence of such entities and so they must exist. Similarly, because mathematics is indispensable to contemporary science, some philosophers argue that this means mathematical objects are objective and exist independently of a person’s mind.
Likewise, we suggest that color plays an indispensable role in evolutionary biology. For example, researchers have argued that aposematism – the use of colors to signal a warning for predators – also benefits an animal’s ability to gather resources. Here, an animal’s coloration works directly to expand its food-gathering niche insofar as it informs potential predators that the animal is poisonous or venomous.
In fact, animals can exploit the fact that the same color pattern can be perceived differently by different perceivers. For instance, some damselfish have ultraviolet face patterns that help them be recognized by other members of their species and communicate with potential mates while remaining largely hidden to predators unable to perceive ultraviolet colors.
In sum, our ability to determine whether objects are colored the same or differently and the indispensable roles they play in science suggest that colors are as real and objective as length and temperature.
‘Extraordinary claims require extraordinary evidence’ − an astronomer explains how much evidence scientists need to claim discoveries like extraterrestrial life
The detection of life beyond Earth would be one of the most profound discoveries in the history of science. The Milky Way galaxy alone hosts hundreds of millions of potentially habitable planets. Astronomers are using powerful space telescopes to look for molecular indicators of biology in the atmospheres of the most Earth-like of these planets.
But so far, no solid evidence of life has ever been found beyond the Earth. A paper published in April 2025 claimed to detect a signature of life in the atmosphere of the planet K2-18b. And while this discovery is intriguing, most astronomers – including the paper’s authors – aren’t ready to claim that it means extraterrestrial life exists. A detection of life would be a remarkable development.
The astronomer Carl Sagan used the phrase, “Extraordinary claims require extraordinary evidence,” in regard to searching for alien life. It conveys the idea that there should be a high bar for evidence to support a remarkable claim.
I’m an astronomer who has written a book about astrobiology. Over my career, I’ve seen some compelling scientific discoveries. But to reach this threshold of finding life beyond Earth, a result needs to fit several important criteria.
When is a result important and reliable?
There are three criteria for a scientific result to represent a true discovery and not be subject to uncertainty and doubt. How does the claim of life on K2-18b measure up?
First, the experiment needs to measure a meaningful and important quantity. Researchers observed K2-18b’s atmosphere with the James Webb Space Telescope and saw a spectral feature that they identified as dimethyl sulfide.
On Earth, dimethyl sulfide is associated with biology, in particular bacteria and plankton in the oceans. However, it can also arise by other means, so this single molecule is not conclusive proof of life.
Second, the detection needs to be strong. Every detector has some noise from the random motion of electrons. The signal should be strong enough to have a low probability of arising by chance from this noise.
The K2-18b detection has a significance of 3-sigma, which means it has a 0.3% probability of arising by chance.
That sounds low, but most scientists would consider that a weak detection. There are many molecules that could create a feature in the same spectral range.
The “gold standard” for scientific detection is 5-sigma, which means the probability of the finding happening by chance is less than 0.00006%. For example, physicists at CERN gathered data patiently for two years until they had a 5-sigma detection of the Higgs boson particle, leading to a Nobel Prize one year later in 2013.
The announcement of the discovery of the Higgs boson took decades from the time Peter Higgs first predicted the existence of the particle. Scientists, such as Joe Incandela shown here, waited until they’d reached that 5-sigma level to say, ‘I think we have it.’
Third, a result needs to be repeatable. Results are considered reliable when they’ve been repeated – ideally corroborated by other investigators or confirmed using a different instrument. For K2-18b, this might mean detecting other molecules that indicate biology, such as oxygen in the planet’s atmosphere. Without more and better data, most researchers are viewing the claim of life on K2-18b with skepticism.
Claims of life on Mars
In the past, some scientists have claimed to have found life much closer to home, on the planet Mars.
Over a century ago, retired Boston merchant turned astronomer Percival Lowell claimed that linear features he saw on the surface of Mars were canals, constructed by a dying civilization to transport water from the poles to the equator. Artificial waterways on Mars would certainly have been a major discovery, but this example failed the other two criteria: strong evidence and repeatability.
In 1996, NASA held a press conference where a team of scientists presented evidence for biology in the Martian meteorite ALH 84001. Their evidence included an evocative image that seemed to show microfossils in the meteorite.
However, scientists have come up with explanations for the meteorite’s unusual features that do not involve biology. That extraordinary claim has dissipated.
More recently, astronomers detected low levels of methane in the atmosphere of Mars. Like dimethyl sulfide and oxygen, methane on Earth is made primarily – but not exclusively – by life. Different spacecraft and rovers on the Martian surface have returned conflicting results, where a detection with one spacecraft was not confirmed by another.
The low level and variability of methane on Mars is still a mystery. And in the absence of definitive evidence that this very low level of methane has a biological origin, nobody is claiming definitive evidence of life on Mars.
Claims of advanced civilizations
Detecting microbial life on Mars or an exoplanet would be dramatic, but the discovery of extraterrestrial civilizations would be truly spectacular.
The search for extraterrestrial intelligence, or SETI, has been underway for 75 years. No messages have ever been received, but in 1977 a radio telescope in Ohio detected a strong signal that lasted only for a minute.
This signal was so unusual that an astronomer working at the telescope wrote “Wow!” on the printout, giving the signal its name. Unfortunately, nothing like it has since been detected from that region of the sky, so the Wow! Signal fails the test of repeatability.
In 2017, a rocky, cigar-shaped object called ‘Oumuamua was the first known interstellar object to visit the solar system. ‘Oumuamua’s strange shape and trajectory led Harvard astronomer Avi Loeb to argue that it was an alien artifact. However, the object has already left the solar system, so there’s no chance for astronomers to observe it again. And some researchers have gathered evidence suggesting that it’s just a comet.
While many scientists think we aren’t alone, given the enormous amount of habitable real estate beyond Earth, no detection has cleared the threshold enunciated by Carl Sagan.
Claims about the universe
These same criteria apply to research about the entire universe. One particular concern in cosmology is the fact that, unlike the case of planets, there is only one universe to study.
A cautionary tale comes from attempts to show that the universe went through a period of extremely rapid expansion a fraction of a second after the Big Bang. Cosmologists call this event inflation, and it is invoked to explain why the universe is now smooth and flat.
In 2014, astronomers claimed to have found evidence for inflation in a subtle signal from microwaves left over after the Big Bang. Within a year, however, the team retracted the result because the signal had a mundane explanation: They had confused dust in our galaxy with a signature of inflation.
On the other hand, the discovery of the universe’s acceleration shows the success of the scientific method. In 1929, astronomer Edwin Hubble found that the universe was expanding. Then, in 1998, evidence emerged that this cosmic expansion is accelerating. Physicists were startled by this result.
Two research groups used supernovae to separately trace the expansion. In a friendly rivalry, they used different sets of supernovae but got the same result. Independent corroboration increased their confidence that the universe was accelerating. They called the force behind this accelerating expansion dark energy and received a Nobel Prize in 2011 for its discovery.
On scales large and small, astronomers try to set a high bar of evidence before claiming a discovery.
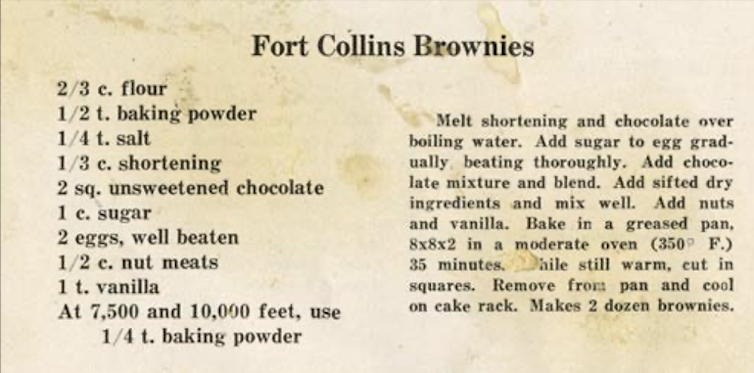
Many bakers working at high altitudes have carefully followed a standard recipe only to reach into the oven to find a sunken cake, flat cookies or dry muffins.
Experienced mountain bakers know they need a few tricks to achieve the same results as their fellow artisans working at sea level.
These tricks are more than family lore, however. They originated in the early 20th century thanks to research on high-altitude baking done by Inga Allison, then a professor at Colorado State University. It was Allison’s scientific prowess and experimentation that brought us the possibility of perfect high-altitude brownies and other baked goods.
We are two current academics at CSU whose work has been touched by Allison’s legacy.
One of us – Caitlin Clark – still relies on Allison’s lessons a century later in her work as a food scientist in Colorado. The other – Tobi Jacobi – is a scholar of women’s rhetoric and community writing, and an enthusiastic home baker in the Rocky Mountains, who learned about Allison while conducting archival research on women’s work and leadership at CSU.
Inga Allison is one of the fascinating and accomplished women who is part of the exhibit.
Allison was born in 1876 in Illinois and attended the University of Chicago, where she completed the prestigious “science course” work that heavily influenced her career trajectory. Her studies and research also set the stage for her belief that women’s education was more than preparation for domestic life.
In 1908, Allison was hired as a faculty member in home economics at Colorado Agricultural College, which is now CSU. She joined a group of faculty who were beginning to study the effects of altitude on baking and crop growth. The department was located inside Guggenheim Hall, a building that was constructed for home economics education but lacked lab equipment or serious research materials.
Allison took both the land grant mission of the university with its focus on teaching, research and extension and her particular charge to prepare women for the future seriously. She urged her students to move beyond simple conceptions of home economics as mere preparation for domestic life. She wanted them to engage with the physical, biological and social sciences to understand the larger context for home economics work.
Such thinking, according to CSU historian James E. Hansen, pushed women college students in the early 20th century to expand the reach of home economics to include “extension and welfare work, dietetics, institutional management, laboratory research work, child development and teaching.”
News articles from the early 1900s track Allison giving lectures like “The Economic Side of Natural Living” to the Colorado Health Club and talks on domestic science to ladies clubs and at schools across Colorado. One of her talks in 1910 focused on the art of dishwashing.
Allison became the home economics department chair in 1910 and eventually dean. In this leadership role, she urged then-CSU President Charles Lory to fund lab materials for the home economics department. It took 19 years for this dream to come to fruition.
In the meantime, Allison collaborated with Lory, who gave her access to lab equipment in the physics department. She pieced together equipment to conduct research on the relationship between cooking foods in water and atmospheric pressure, but systematic control of heat, temperature and pressure was difficult to achieve.
She sought other ways to conduct high-altitude experiments and traveled across Colorado where she worked with students to test baking recipes in varied conditions, including at 11,797 feet in a shelter house on Fall River Road near Estes Park.
But Allison realized that recipes baked at 5,000 feet in Fort Collins and Denver simply didn’t work in higher altitudes. Little advancement in baking methods occurred until 1927, when the first altitude baking lab in the nation was constructed at CSU thanks to Allison’s research. The results were tangible — and tasty — as public dissemination of altitude-specific baking practices began.
As a senior food scientist in a mountain state, one of us – Caitlin Clark – advises bakers on how to adjust their recipes to compensate for altitude. Thanks to Allison’s research, bakers at high altitude today can anticipate how the lower air pressure will affect their recipes and compensate by making small adjustments.
Air pressure is a force that pushes back on all of the molecules in a system and prevents them from venturing off into the environment. Heat plays the opposite role – it adds energy and pushes molecules to escape.
When water is boiled, molecules escape by turning into steam. The less air pressure is pushing back, the less energy is required to make this happen. That’s why water boils at lower temperatures at higher altitudes – around 200 degrees Fahrenheit in Denver compared with 212 F at sea level.
So, when baking is done at high altitude, steam is produced at a lower temperature and earlier in the baking time. Carbon dioxide produced by leavening agents also expands more rapidly in the thinner air. This causes high-altitude baked goods to rise too early, before their structure has fully set, leading to collapsed cakes and flat muffins. Finally, the rapid evaporation of water leads to over-concentration of sugars and fats in the recipe, which can cause pastries to have a gummy, undesirable texture.
Allison was one of many groundbreaking women in the early 20th century who actively supported higher education for women and advanced research in science, politics, humanities and education in Colorado.
Others included Grace Espy-Patton, a professor of English and sociology at CSU from 1885 to 1896 who founded an early feminist journal and was the first woman to register to vote in Fort Collins. Miriam Palmer was an aphid specialist and master illustrator whose work crafting hyper-realistic wax apples in the early 1900s allowed farmers to confirm rediscovery of the lost Colorado Orange apple, a fruit that has been successfully propagated in recent years.
In 1945, Allison retired as both an emerita professor and emerita dean at CSU. She immediately stepped into the role of student and took classes in Russian and biochemistry.
In the fall of 1958, CSU opened a new dormitory for women that was named Allison Hall in her honor.





























































{kind=link}
{kind=link}