Without urgent intervention, our study forecasts that more than 80% of adults and close to 60% of adolescents will be classified as overweight or obese by 2050. These are the key findings of our recent study, published in the journal The Lancet.
Synthesizing body mass index data from 132 unique sources in the U.S., including national and state-representative surveys, we examined the historical trend of obesity and the condition of being overweight from 1990 to 2021 and forecast estimates through 2050.
For people 18 and older, the condition health researchers refer to as “overweight” was defined as having a body mass index, or BMI, of 25 kilograms per square meter (kg/m²) to less than 30 kg/m² and obesity as a BMI of 30 kg/m² or higher. For those younger than 18, we based definitions on the International Obesity Task Force criteria.
This study was conducted by the Global Burden of Disease Study 2021 U.S. Obesity Forecasting Collaborator Group, which comprises over 300 experts and researchers specializing in obesity.
There are ways to combat the trends, such as making activity fun and leading by example.
Obesity has slowed health improvements and life expectancy in the U.S. compared with other high-income nations. Previous research showed that obesity accounted for 335,000 deaths in 2021 alone and is one of the most dominant and fastest-growing risk factors for poor health and early death. Obesity increases the risk of diabetes, heart attack, stroke, cancer and mental health disorders.
The economic implications of obesity are also profound. A report by Republican members of the Joint Economic Committee of the U.S. Congress, published in 2024, predicted that obesity-related health care costs will rise to US$9.1 trillion over the next decade.
The rise in childhood and adolescent obesity is particularly concerning, with the rate of obesity more than doubling among adolescents ages 15 to 24 since 1990. Data from the National Health and Nutrition Examination Survey revealed that nearly 20% of children and adolescents in the U.S. ages 2 to 19 live with obesity.
By 2050, our forecast results suggest that 1 in 5 children and 1 in 3 adolescents will experience obesity. The increase in obesity among children and adolescents not only triggers the early onset of chronic diseases but also negatively affects mental health, social interactions and physical functioning.
What other research is being done
Our research highlighted substantial geographical disparities in overweight and obesity prevalence across states, with southern U.S. states observing some of the highest rates.
Other studies on obesity in the United States have also underscored significant socioeconomic, racial and ethnic disparities. Previous studies suggest that Black and Hispanic populations exhibit higher obesity rates compared with their white counterparts. These disparities are further exacerbated by systemic barriers, including discrimination, unequal access to education, health care and economic inequities.
Furthermore, there is a growing body of research examining technology-driven behavioral interventions, such as mobile health apps, to support weight management. However, whether many of these programs are scalable and sustainable is not yet clear. This gap hinders the broader adoption and adaptation of effective interventions, limiting their potential impact at the population level.
What’s next
Our study forecasts trends in overweight and obesity prevalence over the next three decades, from 2022 to 2050, assuming no action is taken.
With the advent of new-generation anti-obesity medications, obesity management could change substantially. However, the extent of this impact will depend on factors such as cost, accessibility, coverage, long-term efficacy and variability in individual responses. Future research will need to leverage the most up-to-date evidence.
The Research Brief is a short take on interesting academic work.
Political chasms, wars, oppression … it’s easy to feel hopeless and helpless watching these dark forces play out. Could any of us ever really make a meaningful difference in the face of so much devastation?
Given the scale of the world’s problems, it might feel like the small acts of human connection and solidarity that you do have control over are like putting Band-Aids on bullet wounds. It can feel naive to imagine that small acts could make any global difference.
As a psychologist, human connection researcher and audience member, I was inspired to hear musician Hozier offer a counterpoint at a performance this year. “The little acts of love and solidarity that we offer each other can have powerful impact … ” he told the crowd. “I believe the core of people on the whole is good – I genuinely do. I’ll die on that hill.”
I’m happy to report that the science agrees with him.
Research shows that individual acts of kindness and connection can have a real impact on global change when these acts are collective. This is true at multiple levels: between individuals, between people and institutions, and between cultures.
This relational micro-activism is a powerful force for change – and serves as an antidote to hopelessness because unlike global-scale issues, these small acts are within individuals’ control.
A personal connection makes you more willing to find common ground.
Theoretically, the idea that small, interpersonal acts have large-scale impact is explained by what psychologists call cognitive dissonance: the discomfort you feel when your actions and beliefs don’t line up.
For example, imagine two people who like each other. One believes that fighting climate change is crucial, and the other believes that climate change is a political ruse. Cognitive dissonance occurs: They like each other, but they disagree. People crave cognitive balance, so the more these two like each other, the more motivated they will be to hear each other out.
According to this model, then, the more you strengthen your relationships through acts of connection, the more likely you’ll be to empathize with those other individual perspectives. When these efforts are collective, they can increase understanding, compassion and community in society at large. Issues like war and oppression can feel overwhelming and abstract, but the abstract becomes real when you connect to someone you care about.
So, does this theory hold up when it comes to real-world data?
Small acts of connection shift attitudes
Numerous studies support the power of individual acts of connection to drive larger-scale change.
For instance, researchers studying the political divide in the U.S. found that participants self-identifying as Democrats or Republicans “didn’t like” people in the other group largely due to negative assumptions about the other person’s morals. People also said they valued morals like fairness, respect, loyalty and a desire to prevent harm to others.
I’m intentionally leaving out which political group preferred which traits – they all sound like positive attributes, don’t they? Even though participants thought they didn’t like each other based on politics, they also all valued traits that benefit relationships.
One interpretation of these findings is that the more people demonstrate to each other, act by act, that they are loyal friends and community members who want to prevent harm to others, the more they might soften large-scale social and political disagreements.
Even more convincingly, another study found that Hungarian and Romanian students – people from ethnic groups with a history of social tensions – who said they had strong friendships with each other also reported improved attitudes toward the other group. Having a rocky friendship with someone from the other group actually damaged attitudes toward the other ethnic group as a whole. Again, nurturing the quality of relationships, even on an objectively small scale, had powerful implications for reducing large-scale tensions.
In another study, researchers examined prejudice toward what psychologists call an out-group: a group that you don’t belong to, whether based on ethnicity, political affiliation or just preference for dogs versus cats.
They asked participants to reflect on the positive qualities of someone they knew, or on their own positive characteristics. When participants wrote about the positive qualities of someone else, rather than themselves, they later reported lower levels of prejudice toward an out-group – even if the person they wrote about had no connection to that out-group. Here, moving toward appreciation of the other, rather than away from prejudice, was an effective way to transform preconceived beliefs.
So, small acts of connection can shift personal attitudes. But can they really affect societies?
From one-on-one to society-wide
Every human being is embedded in their own network with the people and world around them, what psychologists call their social ecology. Compassionate change at any level of someone’s social ecology – internally, interpersonally or structurally – can affect all the other levels, in a kind of positive feedback loop, or upward spiral.
For instance, both system-level anti-discrimination programming in schools and interpersonal support between students act reciprocally to shape school environments for students from historically marginalized groups. Again, individual acts play a key role in these positive domino effects.
Small positive steps can build off each other in a chain reaction.
Even as a human connection researcher, I’ve been surprised by how much I and others have progressed toward mutual understanding by simply caring about each other. But what are small acts of connection, after all, but acts of strengthening relationships, which strengthen communities, which influence societies?
In much of my clinical work, I use a model called social practice — or “intentional community-building” – as a form of therapy for people recovering from serious mental illnesses, like schizophrenia. And if intentional community-building can address some of the most debilitating states of the human psyche, I believe it follows that, writ large, it could help address the most debilitating states of human societies as well.
Simply put, science supports the idea that moving toward each other in small ways can be transformational. I’ll die on that hill too.
The Food and Drug Administration issued three alerts throughout 2024, warning consumers about lead in certain brands of cinnamon products. Such notices rightfully put consumers on alert and have people wondering if the spice products they buy are safe – or not.
A Consumer Reports investigation of more than three dozen ground cinnamon products found that 1 in 3 contain lead levels above 1 part per million.
There are several things consumers should be thinking about when it comes to lead – and other heavy metals – in cinnamon.
Why is lead found in cinnamon?
Most people are familiar with cinnamon in two forms – sticks and ground spice. Both come from the dried inner bark of the cinnamon tree, which is harvested after a few years of cultivation. For the U.S. market, cinnamon is largely imported from Indonesia, Vietnam, Sri Lanka, India and China.
One way that lead could accumulate in cinnamon tree bark is when trees are cultivated in contaminated soil. Lead can also be introduced in cinnamon products during processing, such as grinding.
When ground cinnamon is prepared, some producers may add lead compounds intentionally to enhance the weight or color of the product and, thus, fetch a higher sale price. This is known as “food adulteration,” and products with known or suspected adulteration are refused entry into the U.S.
However, in the fall of 2023, approximately 600 cases of elevated blood lead levels in the U.S., defined as levels equal to or above 3.5 micrograms per deciliter – mostly among children – were linked to the consumption of certain brands of cinnamon apple sauce. The levels of lead in cinnamon used to manufacture those products ranged from 2,270 to 5,110 parts per million, indicating food adulteration. The manufacturing plant was investigated by the FDA.
Cinnamon trees in Zanzibar, Tanzania. Zanzibar is known the world over as the ‘spice islands.’
There are no federal guidelines for lead or other heavy metals in spices. New York state has proposed even stricter guidelines than its current level of 1 part per million, which would allow the New York Department of Agriculture and Markets to remove products from commerce if lead levels exceed 0.21 parts per million.
What does it mean that ‘the dose makes the poison’?
The lead dose we are exposed to from foods depends on the level of lead in the food and how much of that food we eat. Higher doses mean more potential harm. The frequency with which we consume foods – meaning daily versus occasionally – also matters.
For spices like cinnamon, the amount and frequency of consumption depends on cultural traditions and personal preference. For many, cinnamon is a seasonal spice; others use it year-round in savory dishes or sauces.
Cinnamon is beloved in baked goods. Take a cinnamon roll recipe calling for 1.5 tablespoons (slightly less than 12 grams) of the spice. If a recipe yields 12 rolls, each will have around 1 gram of cinnamon. In the Consumer Reports investigation, some cinnamon products were classified as “okay to use” or “best to use.”
The highest value of lead in cinnamon products in the “okay to use” category was 0.87 parts per million, and in the “best to use” category, it was 0.15 parts per million. A child would have to consume 2.5 or more rolls made with the “okay to use” cinnamon to exceed the FDA guideline on limiting lead intake from foods to 2.2 micrograms per day, assuming that no other food contained lead. To exceed this guideline with “best to use” cinnamon, a child would have to eat 15 or more rolls.
Research suggests that ground cinnamon contains higher lead levels than cinnamon sticks.
Can cinnamon contribute to elevated blood lead levels?
Because of lead’s effects on development in early life, the greatest concern is for exposure in young children and pregnant women. Lead is absorbed in the small intestine, where it can latch onto cellular receptors that evolved to carry iron and other metals.
The impact of a contaminated spice on a person’s blood lead level depends on the dose of exposure and the proportion of lead available for intestinal absorption. For several spices, the proportion of available lead was 49%, which means that about half of the lead that is ingested will be absorbed.
People who have nutritional deficiencies, such as iron deficiency, also tend to absorb more lead and have higher blood lead levels. This is because our bodies compensate for the deficiency by producing more receptors to capture iron from foods. Lead takes advantage of the additional receptors to enter the body. Young children and pregnant women are at higher risk for developing iron deficiency, so there is good reason for vigilance about lead in the foods they consume.
Studies show that among children with lead poisoning in the U.S., contaminated spices were one of several sources of lead exposure. Studies that estimate blood lead levels from statistical models suggest that consuming 5 micrograms of lead or more from spices daily could substantially contribute to elevated blood lead levels.
For occasional or seasonal consumption, or lower levels of contamination, more research is needed to understand how lead in spices would affect lead levels in the blood.
For people who have other sources of lead in their homes, jobs or hobbies, additional lead from foods or spices may matter more because it adds to the cumulative dose from multiple exposure sources.
How to test for elevated blood lead levels
The Centers for Disease Control and Prevention recommends that children at risk for lead exposure get a blood lead test at 1 and 2 years of age. Older children can also get tested. Finger-prick screening tests are often available in pediatric offices, but results may need to be confirmed in venous blood if the screening result was elevated.
Adults in the U.S. are not routinely tested for lead exposure, but concerned couples who plan on having children should talk to their health care providers.
What to consider when using or buying cinnamon or other spices
Does your household use spices frequently and in large amounts?
Do young children or pregnant women in your household consume spices?
Do you typically consume spices on breakfast foods or beverages?
If the answer to any of these questions is yes, then buy good-quality products, from large, reputable sellers. Think about using cinnamon sticks if possible.
Medicare Advantage – the commercial alternative to traditional Medicare – is drawing down federal health care funds, costing taxpayers an extra 22% per enrollee to the tune of US$83 billion a year.
Medicare Advantage, also known as Part C, was supposed to save the government money. The competition among private insurance companies, and with traditional Medicare, to manage patient care was meant to give insurance companies an incentive to find efficiencies. Instead, the program’s payment rules overpay insurance companies on the taxpayer’s dime.
We are health carepolicy experts who study Medicare, including how the structure of the Medicare payment system is, in the case of Medicare Advantage, working against taxpayers.
Medicare beneficiaries choose an insurance plan when they turn 65. Younger people can also become eligible for Medicare due to chronic conditions or disabilities. Beneficiaries have a variety of options, including the traditional Medicare program administered by the U.S. government, Medigap supplements to that program administered by private companies, and all-in-one Medicare Advantage plans administered by private companies.
Researchers have found that the overpayment to Medicare Advantage companies, which has grown over time, was, intentionally or not, baked into the Medicare Advantage payment system. Medicare Advantage plans are paid more for enrolling people who seem sicker, because these people typically use more care and so would be more expensive to cover in traditional Medicare.
Some of this extra money is spent to lower cost sharing, lower prescription drug premiums and increase supplemental benefits like vision and dental care. Though Medicare Advantage enrollees may like these benefits, funding them this way is expensive. For every extra dollar that taxpayers pay to Medicare Advantage companies, only roughly 50 to 60 cents goes to beneficiaries in the form of lower premiums or extra benefits.
As Medicare Advantage becomes increasingly expensive, the Medicare program continues to face funding challenges.
In our view, in order for Medicare to survive long term, Medicare Advantage reform is needed. The way the government pays the private insurers who administer Medicare Advantage plans, which may seem like a black box, is key to why the government overpays Medicare Advantage plans relative to traditional Medicare.
The current Medicare Advantage payment system, implemented in 2006 and heavily reformed by the Affordable Care Act in 2010, had two policy goals. It was designed to encourage private plans to offer the same or better coverage than traditional Medicare at equal or lesser cost. And, to make sure beneficiaries would have multiple Medicare Advantage plans to choose from, the system was also designed to be profitable enough for insurers to entice them to offer multiple plans throughout the country.
To accomplish this, Medicare established benchmark estimates for each county. This benchmark calculation begins with an estimate of what the government-administered traditional Medicare plan would spend on the average county resident. This value is adjusted based on several factors, including enrollee location and plan quality ratings, to give each plan its own benchmark.
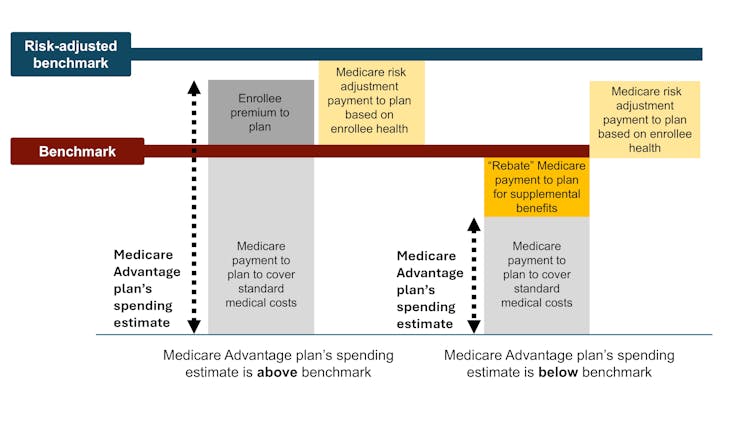
Medicare Advantage plans then submit bids, or estimates, of what they expect their plans to spend on the average county enrollee. If a plan’s spending estimate is above the benchmark, enrollees pay the difference as a Part C premium.
Most plans’ spending estimates are below the benchmark, however, meaning they project that the plans will provide coverage that is equivalent to traditional Medicare at a lower cost than the benchmark. These plans don’t charge patients a Part C premium. Instead, they receive a portion of the difference between their spending estimate and the benchmark as a rebate that they are supposed to pass on to their enrollees as extras, like reductions in cost-sharing, lower prescription drug premiums and supplemental benefits.
The government pays Medicare Advantage plans based on Medicare’s cost estimates for a given county. The benchmark is an estimate from the Centers for Medicare & Medicaid Services of what it would cost to cover an average county enrollee in traditional Medicare, plus adjustments including quartile payments and quality bonuses. The risk-adjusted benchmark also takes into consideration an enrollee’s health.
In theory, this payment system should save the Medicare system money because the risk-adjusted benchmark that Medicare estimates for each plan should run, on average, equal to what Medicare would actually spend on a plan’s enrollees if they had enrolled in traditional Medicare instead.
In reality, the risk-adjusted benchmark estimates are far above traditional Medicare costs. This causes Medicare – really, taxpayers – to spend more for each person who is enrolled in Medicare Advantage than if that person had enrolled in traditional Medicare.
Why are payment estimates so high? There are two main culprits: benchmark modifications designed to encourage Medicare Advantage plan availability, and risk adjustments that overestimate how sick Medicare Advantage enrollees are.
High risk-adjusted benchmarks lead to overpayments from the government to the private companies that administer Medicare Advantage plans.
In 2012, as part of the Affordable Care Act, Medicare Advantage benchmark estimates received another layer: “quartile adjustments.” These made the benchmark estimates, and therefore payments to Medicare Advantage companies, higher in areas with low traditional Medicare spending and lower in areas with high traditional Medicare spending. This benchmark adjustment was meant to encourage more equitable access to Medicare Advantage options.
In that same year, Medicare Advantage plans started receiving “quality bonus payments” with plans that have higher “star ratings” based on quality factors such as enrollee health outcomes and care for chronic conditions receiving higher bonuses.
Even before fully taking into account risk adjustment, recent estimates peg the benchmarks, on average, as 8% higher than average traditional Medicare spending. This means that a Medicare Advantage plan’s spending estimate could be below the benchmark and the plan would still get paid more for its enrollees than it would have cost the government to cover those same enrollees in traditional Medicare.
Overestimating enrollee sickness
The second major source of overpayment is health risk adjustment, which tends to overestimate how sick Medicare Advantage enrollees are.
Each year, Medicare studies traditional Medicare diagnoses, such as diabetes, depression and arthritis, to understand which have higher treatment costs. Medicare uses this information to adjust its payments for Medicare Advantage plans. Payments are lowered for plans with lower predicted costs based on diagnoses and raised for plans with higher predicted costs. This process is known as risk adjustment.
But there is a critical bias baked into risk adjustment. Medicare Advantage companies know that they’re paid more if their enrollees seem more sick, so they diligently make sure each enrollee has as many diagnoses recorded as possible.
This can include legal activities like reviewing enrollee charts to ensure that diagnoses are recorded accurately. It can also occasionally entail outright fraud, where charts are “upcoded” to include diagnoses that patients don’t actually have.
In traditional Medicare, most providers – the exception being Accountable Care Organizations – are not paid more for recording diagnoses. This difference means that the same beneficiary is likely to have fewer recorded diagnoses if they are enrolled in traditional Medicare rather than a private insurer’s Medicare Advantage plan. Policy experts refer to this phenomenon as a difference in “coding intensity” between Medicare Advantage and traditional Medicare.
The same person is likely to be documented with more illnesses if they enroll in Medicare Advantage rather than traditional Medicare – and cost taxpayers more money.
The differences in coding and favorable selection make beneficiaries look sicker when they enroll in Medicare Advantage instead of traditional Medicare. This makes cost estimates higher than they should be. Research shows that this mismatch – and resulting overpayment – is likely only going to get worse as Medicare Advantage grows.
It also makes it difficult for traditional Medicare to compete with Medicare Advantage.
Traditional Medicare, which tends to cost the Medicare program less per enrollee, is only allowed to provide the standard Medicare benefits package. If its enrollees want dental coverage or hearing aids, they have to purchase these separately, alongside a Part D plan for prescription drugs and a Medigap plan to lower their deductibles and co-payments.
Medicare Advantage plans offer extras, but at a high cost to the Medicare system – and taxpayers. Only 50-60 cents of a dollar spent is returned to enrollees as decreased costs or increased benefits.
The system sets up Medicare Advantage plans to not only be overpaid but also be increasingly popular, all on the taxpayers’ dime. Plans heavily advertise to prospective enrollees who, once enrolled in Medicare Advantage, will likely have difficulty switching into traditional Medicare, even if they decide the extra benefits are not worth the prior authorization hassles and the limited provider networks. In contrast, traditional Medicare typically does not engage in as much direct advertising. The federal government only accounts for 7% of Medicare-related ads.
There is a long-running debate over what type of coverage should be required under both traditional Medicare and Medicare Advantage. Recently, policy experts have advocated for introducing an out-of-pocket maximum to traditional Medicare. There have also been multiple unsuccessfulefforts to make dental, vision, and hearing services part of the standard Medicare benefits package.
Although all older people require regular dental care and many of them require hearing aids, providing these benefits to everyone enrolled in traditional Medicare would not be cheap. One approach to providing these important benefits without significantly raising costs is to make these benefits means-tested. This would allow people with lower incomes to purchase them at a lower price than higher-income people. However, means-testing in Medicare can be controversial.
There is also debate over how much Medicare Advantage plans should be allowed to vary. The average Medicare beneficiary has over 40 Medicare Advantage plans to choose from, making it overwhelming to compare plans. For instance, right now, the average person eligible for Medicare would have to sift through the fine print of dozens of different plans to compare important factors, such as out-of-pocket maximums for medical care, coverage for dental cleanings, cost-sharing for inpatient stays, and provider networks.
Although millions of people are in suboptimal plans, 70% of people don’t even compare plans, let alone switch plans, during the annual enrollment period at the end of the year, likely because the process of comparing plans and switching is difficult, especially for older Americans.
MedPAC, a congressional advising committee, suggests that limiting variation in certain important benefits, like out-of-pocket maximums and dental, vision and hearing benefits, could help the plan selection process work better, while still allowing for flexibility in other benefits. The challenge is figuring out how to standardize without unduly reducing consumers’ options.
The Medicare Advantage program enrolls over half of Medicare beneficiaries. However, the $83-billion-per-year overpayment of plans, which amounts to more than 8% of Medicare’s total budget, isunsustainable. We believe the Medicare Advantage payment system needs a broad reform that aligns insurers’ incentives with the needs of Medicare beneficiaries and American taxpayers.
This article is part of an occasional series examining the U.S. Medicare system.